Stack Exchange network consists of 183 Q&A communities including Stack Overflow, the largest, most trusted online community for developers to learn, share their knowledge, and build their careers.
A new study published in the New England Journal of Medicine (NEJM) shows not only that the effectiveness of the Pfizer Covid vaccine becomes negative (meaning the vaccinated are more likely to be infected than the unvaccinated) within five months but that the vaccine destroys any protection a person has from natural immunity.
The study is a large observational study that looks at 887,193
children aged 5 to 11 years in North Carolina, of whom 273,157 (30.8%)
received at least one dose of Pfizer vaccine between November 1st 2021
and June 3rd 2022. The study includes 193,346 SARS-CoV-2 infections
reported between March 11th 2020 and June 3rd 2022.
The researchers used a form of statistical modelling with adjustments
for confounding factors (such as underlying conditions) to calculate
estimates of vaccine effectiveness over time and against the different
Covid variants.
The findings are depicted in the charts below. In chart A, notice that
the green and blue lines, representing children vaccinated in November
and December respectively, go through zero into negative territory at
a sharp gradient within five months of the first injection. It’s
unclear why the green line is not continued past April, as the
researchers presumably had the data, but from what is shown it looks
very much like the vaccine effectiveness will continue declining deep
into negative territory.
[...]
Does the Pfizer vaccine destroy natural immunity in children?
Also, worth noting that negative vaccine-effectiveness isn't an unexpected result. For exampe, common depictions of "flattening the curve" (e.g., this image from Wikipedia) tend to show that early-mitigation strategies can lead to (temporarily) higher incidence-rates later on, where the flattened-curve rises above the non-flattened-curve.
@AaarghZombies: Yeah, that makes sense for SE.Skeptics and in terms of cultural impact. I just meant that it might be hard to find a reputable reference about stuff like negative vaccine-effectiveness due to the cultural noise.
(To be clear, a very reasonable response to the question would be: The phrase "vaccine effectiveness" used in the paper does not in fact correspond to any real-world concept that any lay person would recognise as having anything to do with the effectiveness of a vaccine. This applies whether or not the paper has been mis-quoted.)
If you read the original, rather short article you'll notice that it never makes any kind of claim about the vaccine destroying any protection. To the contrary, the article argues that the data supports booster vaccinations for children.
Reuters has done a fact check of this claim which includes quotes from the original author of the study.
“The statement that ‘the vaccine destroys any protection a person has from natural immunity’ is unfounded,” Lin told Reuters in an email. “Our data showed that the vaccine was effective against infection for 4 months. In addition, vaccination conferred greater protection against hospitalization than against infection. Finally, no vaccinated children died whereas 7 unvaccinated children died.”
So the author of the study used to make this claim directly refutes it.
In both figures, the lines’ continuation past the boundaries of the graph is strictly an illustrative technique, to show the overall trajectory more clearly, according to Lin. They do not indicate that vaccine effectiveness becomes “negative” at any point, or that children become more vulnerable to infection than they would be without vaccination, he said.
I really dislike these graphs, they don't show clearly which parts are actual data points and which parts are interpolated or extrapolated. But no matter how bad these graphs are, according to the author they are not intended to show that the vaccines reduce protection, that is simply an extrapolated line and not measured data.
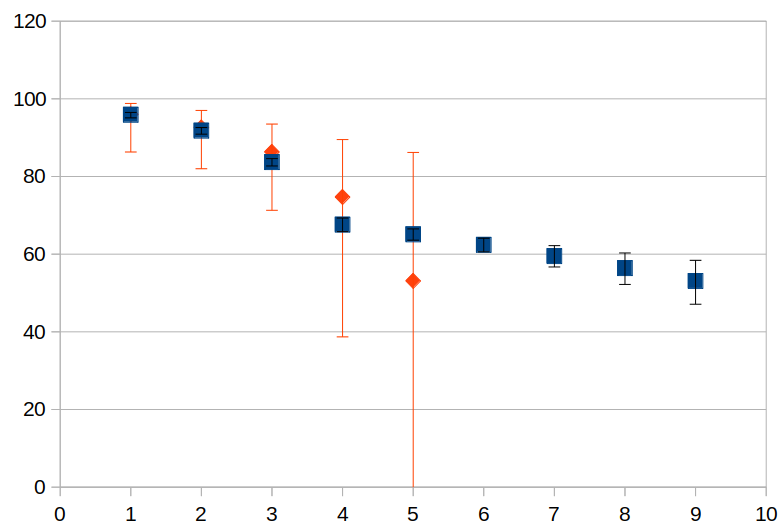
As for the graphs C&D, they are very hard to read in my opinion as they don't clearly indicate which points of data were measured (which are fewer for the vaccinated case than for the unvaccinated case, so the timeframe observered is different in both cases). The error bars are also somewhat confusing as there is also the shading for the prevalence of the different mutations in the background. I created a very rough plot myself from the data in the supplementary material (only for the delta variant) to understand this:
Blue are the unvaccinated, red the vaccinated children. The x-axis is the number of months.
The error bars for the vaccinated children are much, much larger than the error bars for the unvaccinated children. The series also doesn't continue as long as it does for the unvaccinated children. The "trend" you see in graph D for the vaccinated children seems to be an extrapolation that is based mostly on the last two data points that have absolutely enormous error bars. This is extremely misleading and not at all what the raw data shows.
Their supplementary-materials (PDF) explains their methods a bit. Looks like it's basically a lot of estimates throughout. And apparently they tweaked the results to look more reasonable -- e.g., "We consider change points at every 4, 5 or 6 weeks but may omit change points near the end to improve stability of estimation.". Given the level of manipulation involved, it might be reasonable to interpret those plots as extrapolations throughout (rather than just toward the end).
"If you read the original, rather short article you'll notice that it never makes any kind of claim about the vaccine destroying any protection." That's just false. Charts are claims. And the charts do make that claim. Just because the text doesn't make the claim, and the charts' misinformation was unintentional, doesn't change that. People need to take responsible for what their articles communicate. "But no matter how bad these graphs are, according to the author they are not intended to show that the vaccines reduce protection" Intentions are not dispositive.
@Nat Hmm, that type of data manipulations smells like very shoddy science indeed. I can understand losing precision as time goes on, but improve stability of the estimation sounds an awful lot like "manipulated the data until the results looked good/as desired" I think its especially dishonest to put confidence intervals on the chart when you've explicitly removed data for the sole purpose of making the estimates look more precise/shrinking said CI. If the estimates become unstable that should be reflected in the CI instead of removed.
@MadScientist Did you look at panels C and D in the paper? Unless I'm misunderstanding something, panel C is naturally immune kids and panel D is naturally immune kids that were also vaccinated. You can see that the vaccinated group has significantly lower immunity to delta (although the CI is absurdly large) compared to the unvaccinated group. (It's also unclear to me if the previous infection for group D was pre or post vaccination, which may matter)
@Cole: Yeah, you're right, those confidence-intervals seem inappropriate for the reasons you've stated. Plus there's an issue where they seem to think that vaccine-effectiveness was exactly 0% at vaccination-time -- which they claim to have hard-set because, they claim, vaccinations don't do anything immediately. But their data isn't testing vaccinations in a vacuum; rather, they're testing vaccine-effectiveness in a sense that includes social and behavioral effects, which vaccinations can affect, invalidating their argument of 0%, and making the zero-width confidence-bars off.
This is not an answer, rather a comment trying to clear up a misunderstanding pointing out
what the technical term vaccine effectiveness means, and
that/how negative vaccine effectiveness is nothing very special, and
that/how negative vaccine effectiveness does not imply the vaccine "destroys" immunity.
It does not answer the question of potential "destruction" of children's immune system by the vaccine. It only points out that the argumentation chain in the claim is logically flawed. Vaccine effectiveness is the right answer to the wrong question when discussing the effect of the vaccine on immunity.
(Vaccine) effectiveness is rather a surrogate than the vaccine efficacy we'd tend to think it means.
A surrogate is something that can be easily/practically measured and is used in place or as approximation for difficult-to-measure variables of interest (such as vaccine efficacy).
Vaccine efficacy is
probability of $endpoint if vaccinated
VE = 1 - ——————————————————————————————————————————
probability of $endpoint if not vaccinated
in equal exposure settings, i.e., everything else being equal. There are often different sensible $endpoints: getting infected, getting hospitalized, dying, ...
Thus, vaccine efficacy measures the effect of the vaccine only.
In contrast, vaccine effectiveness is used (according to the Wiki page linked above) when observing effects in a real-world population. This means, besides efficacy it includes selection biases and all kinds of confounders that correlate with vaccine uptake.
The "effectiveness" in the paper is basically
case rate in vaccinated [recovered] population
1 - ——————————————————————————————————————————————
case rate in never-exposed population
(case rate is a surrogate for incidence: the rate of officially counted cases rather than the rate of actual infections)
Now, every factor that happens to change incidence differently in vaccinated vs. never-exposed will be confounding vaccine effectiveness.
The study also explicitly says "Our study is limited by unmeasured confounding and underreporting of Covid-19 cases"
In the supplementary material they list sex, race/ethinicity, geographical region, and county-level vaccination rate as included in their model, but I did not find the corresponding estimates in the letter nor in the supplement.
Now, here's a plausible scenario that can easily lead to such observations even with moderately effective vaccines. We cannot conclude that this is indeed the case, but we can conclude that the observations do not imply "destroyed [or reduced] natural immunity".
Consider the following scenario:
a vaccine that protects well against severe disease*, but is
only moderately effective against infection. Say, true efficacy against infection 67 %, i.e. due to vaccination 2 out of every 3 infections that would occur in unvaccinated are avoided. That's roughly the top estimate in graph B.
The original Wuhan variant had an R0 of roughly 3, i.e. an infected person on average infected 3 susceptible persons when life went on as usual before the pandemic.
With the personal and legally prescibed measures (non-pharmaceutical interventions, NPIs) to battle down exposure, we got the actual (effective) R down to around 1 in 2020 (i.e., before vaccines were available, and when there was no widespread immunity from previous infections in the general population). I.e., those measures mainly of contact reduction were also able to avoid 2 out of every 3 infections that would otherwise have occured.
Now consider people replacing those NPIs by the vaccination. I.e., one gets vaccinated in order to not need to reduce contacts any more. If everyone who is vaccinated in parallel goes back to pre-pandemic contacts, the observed effectiveness against infection would be 0. Slighly lower vaccine efficacy, or also a slight increase in contacts over pre-pandemic level (to catch up) would easily lead to observed negative effectiveness.
* We don't even need a precise number for our scenario. It is sufficient that people take this level of protection as sufficient to not care (much) about infection any more.
Take home message: when vaccination replaces measures to reduce exposure (such as contact reduction), observed effectiveness cannot be used as approximation for efficacy.
Here's some evidence that people were indeed thinking along the lines of getting vaccinated so that contact reduction is not necessary any more:
COSMO survey in Germany asked people to rate their agreement (scale: 1 -> 7 (totally agree)) with statements about the vaccination at the end of 2020 (section 19.7). Back then,
"it's primarily good to protect my health" got 4.71 points agreement, and
"it's primarily good to reduce the disadvantages I have from the pandemic, such as contact reductions, lockdown" got 4.54 points.
Very good to have this, thank you. I am familiar with this risk compensation concept, but I didn't draw the link because I was unaware of the distinction drawn formally between "effectiveness" and "efficacy". But what do you mean by "NPI"?
@Oddthinking: you'd be right in saying this does not answer the question. Thus, feel free to downvote and/or delete as you like. It is theoretical and purely logical, yes. It is not conjecture, though, in pointing out that the question and several comments draw an implication that is logically flawed, the fallacy stemming from misunderstanding/misinterpreting a correctly used technical term. If you have any constructive suggestions how/where to put clarifications, I'm all ears.